A quick, true story to get you asking the right questions
In 1975, Lucy Russell set herself alight in the courtyard of a church and died at the age of 26. This was the end of a troubled life for Lucy, but she was not alone her older sister was also unwell, as was their mother, both of whom spent time in asylums. Their father, John, was a distinguished politician when young, but later, he too suffered from schizophrenia.
For John s father, the famous philosopher and mathematician Bertrand Russell, this was fulfilment of an earlier prophecy. Before Bertrand s first marriage, his grandmother warned of madness in his and the bride s family which would continue in future generations if they married.
This prophecy was a fear Bertrand carried all his life, and because of it, he only had children with his second wife.
While he remained (relatively) untouched by mental illness, his son and his grandchildren were not as fortunate.
So was his grandmother a clairvoyant witch? If not, why was the family of Bertrand Russell so affected by mental illness?
Environment and genetics: one and one make...
To understand the troubles of Bertrand Russell, we have to ask a question why is anyone affected by mental illness?
A mental illness is a health problem that significantly affects how a person feels, thinks, behaves, and interacts with other people. It is diagnosed according to standardised criteria. The term mental disorder is also used to refer to these health problems.
A mental health problem also interferes with how a person thinks, feels, and behaves, but to a lesser extent than a mental illness. Mental health problems are more common – these include the mental ill health that can be experienced temporarily as a reaction to the stresses of life. While less severe, these may develop into a mental illness if they are not effectively dealt with.
Mental illnesses cause a great deal of suffering to those experiencing them, as well as their families and friends. These problems also appear to be increasing. According to the World Health Organization, depression will be one of the biggest health problems worldwide by the year 2020.
Mental illness is quite common half of Australians will have some form of mental illness at some point in their life, with an estimated 1 in 5 suffering from some form of mental illness right now.
Some conditions are more common that others: looking at the table below you can see in the general population some conditions, like anxiety and depression, are fairly common, while schizophrenia is more rare.
Box 1: Percentage of Australians who (on average) have had particular mental illnesses in the last 12 months.
Condition | Percentage |
| Anxiety disorders | ~15% |
| Depression | ~5% |
| Schizophrenia | ~<1% |
Why a person might get a mental illness is thought to be a combination of their environment and their genetics.
Environmental factors that can trigger mental illness can be stressful life events (like losing your job), health factors (like poor sleep or diet), or even where you live. The list of environmental risk factors is growing all the time – famine, migration, seasons, difficult birth, substance use, unstable home life and more have all been linked in some way to mental illness. Of course, the fact that your mother had a difficult pregnancy doesn t mean you are guaranteed a hard life it is the combination of environment and genetics that determines your mental health. In mental health research this is referred to as the gene-environment interaction model.
Genetics can affect how likely you are to develop a condition, given the right environmental factors. How big a role genetics play is different depending on the condition. Something like a broken leg would be very unlikely to be related to genetics (depending on if you think being accident-prone is inheritable!), compared to eye colour. So it s very unlikely you ll inherit a broken leg from your mum or dad, but you may inherit eye colour.
Mental illness seems to be somewhere in the middle you can inherit a susceptibility to mental illness, but that in no way guarantees you ll get it. Every person is different and the weight of genetics and environment will be different as well.
What s in your genes?
How do we know if we might have a gene mutation that makes us more likely to develop a mental illness? If we know the specific gene or genes responsible such as the HTT gene in Huntington s disease, or BCRA1 for hereditary breast cancer we can directly test someone to know if they have the gene and are at a higher risk of developing the illness. This can help with family planning or preventive health measures (one example is Angelina Jolie, who decided to have a double mastectomy when she learned of her family risk of breast cancer).
For mental illnesses, this isn t as easy it doesn t seem to be that single gene change is found in everyone with the condition. Researchers think it might be the build-up of many different genes that is what causes these conditions. Right now a few specific genes have been identified, but these are usually only found in a small number of people or particular populations. We still lack the knowledge to explain the full picture of genetic risk factors for mental illnesses and therefore it is very difficult to test for genetic risk.
An alternative method is to look at your family history. By doing this you can work out (to a point) if you might be at risk for certain conditions because if they have appeared in people with a similar genetic background to you (like your family) that suggests you may have some of the same genes as well.
Family is not just important for genetics – there is the added risk that you will also tend to share some of your environment with your family (including diet, geography or lifestyle). The good news is that these lifestyle or environmental factors can be managed to reduce the risk of developing the illness.
When thinking about the genes you share with your family it is important to understand that shared genes do not mean shared risk of developing the same illness. For example, even when an identical twin develops schizophrenia there is only a 40-50% chance that their twin will also develop the disorder, even when they share 100% genes and a very similar lifestyle. This may be due for example to different exposure to viruses, stress such as an assault, or the most avoidable risk of all cannabis use.
The easiest way to work this out your family history is to draw a family tree. Here s an example of how a family tree that identifies mental illness might look. You can find a blank copy under ‘Plot your own family tree’.
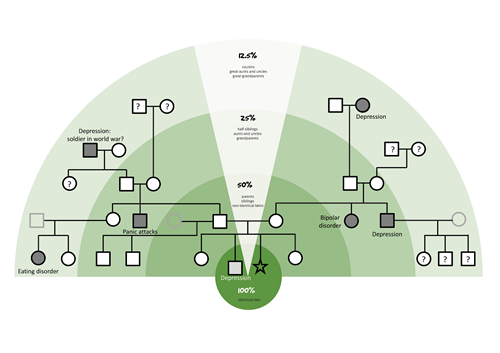
Click picture to enlarge.
When you are finished, examine your family tree. How many relatives do you have with specific conditions? It s likely you ll have a few after all, we already know that mental illnesses are more common than you would think. Compare the percentage of relatives you have to those in box 1 this can give you some idea if you have more relatives unwell than expected.
Also, note how closely related these relatives are to you: the closer they are, the more genetics and/or environment you share, and the stronger your family history of mental illness becomes. If you have a cousin with an eating disorder, this would be less concerning for you than if your sibling has an eating disorder. Your cousin only shares on average one eighth the same genes with you, while your sibling has half – so four times the number of similar genes! A sibling or parent (known as a first degree relative) will share the most genes and environmental factors with you while this is not a promise that you will get a mental illness, it can indicate what specific conditions you might be sensitive to.
Click picture to enlarge.
We have drawn the family tree of the Russell family and Lucy Russell so you can get a better idea of how to read your own family tree. Both sides of her family tree had members with symptoms and behaviours seen in schizophrenia (paranoia, delusions, and hallucinations) which would have given her an even greater genetic risk.
However, it s important to remember that genes are not a jail sentence as far as it s known, the other children and grandchildren of Bertrand Russell seem to have escaped illness so far. Lucy and her sister also had a traumatic childhood, having been taken into Bertrand Russell s care after being abandoned by their parents. It is likely then, that it was a combination of genes and environmental stress that led to mental illness.
Family History: what now?
You might feel a bit down after looking at your family tree, particularly if you seem to have a lot of relatives with mental illness. After all, it is impossible to change your genes, right?
Well, yes and no. It is important to remember that genes are only part of who we are identical twins who share (very almost) identical DNA do not have the same mental health outcomes. For example, studies of identical twins have found that if one twin had bipolar disorder, the other is 30-60% likely to have it as well. For a non-identical twin, it is only 10%. Environment clearly has some role in the occurrence of these conditions.
While there isn t much we can do to our genetics, we do have some control over our environment and behaviours. For instance, someone who has a history of type 2 diabetes in their family can reduce their risk in the future by eating a better diet and exercising regularly now.
Knowing your family history gives you the control to make informed decisions about your environment and be aware of your environmental risk factors.
There are some things you can do:
- Avoid taking psychoactive drugs, particularly during adolescence.
Psychoactive drugs alter brain chemistry. This can be a problem if the brain is still developing, as it is during your teenage years.
During childhood, your brain undergoes the setting up stage by creating lots and lots of connections: when you are 11 or 12, your brain will have the most connections you ll have in your whole life! However, it is still a work-in-progress during the following years, the brain prunes down to keep only the most efficient connections, and then amplifies their signal. There are some estimates that your brain isn t fully developed until your late 20s.
Using drugs that alter brain chemistry during this period increases the risk of interfering with development, especially if they are taken in large amounts and often. This is a problem because teenage years seem to be a particularly sensitive period for mental illness to occur, whether because of developmental changes or the increased environmental stressors. This is even worse if you already have underlying genetics that predispose you to mental illness.
Cannabis seems to act as a multiplier for existing effects and this is more the case the earlier in your teenage years you start using cannabis and the heavier you use it. Evidence has shown cannabis can increase the likelihood of anxiety and depression by up to five times; for mania in bipolar disorder and schizophrenia, it is estimated cannabis can increase the risk by between three and four times. If you already start with an increased genetic risk, it will be much greater when you add cannabis.
Not everyone experiences the same effects when they use cannabis the reasons why may be down to their genetics. You can t always control your environment, but you can control whether or not you choose to use a particular drug, at what age and how much you use.
- Healthy body, healthy mind.
Being physically healthy can be protective against mental illness. This means having good sleep patterns and diet, as well as exercise regularly.
A healthy mind can be harder to achieve however, having particular thought patterns can help us be more resilient (or sensitive) towards environmental stressors. Identifying the negative thoughts patterns and behaviours that are not helpful to our wellbeing is the first step towards improving our mental health.
- Be aware of self-medication good and bad!
Of course, looking after yourself is good when it s done right! Sometimes we can do things to make ourselves feel better in the short-term, but they don t necessarily help us in the long-term.
Self-medication with alcohol or other drugs, like nicotine, is one example of doing something to make ourselves feel better in the short-term. Eating junk food or gaming to excessive degrees can also fall into this category.
This doesn t mean you can t have fun but take note of what you do when you are feeling down or anxious and ask yourself if it is a healthy choice. It can be a good idea to mix up the things you do to give yourself a boost and to know which specifically avoid for example, cannabis use is the most avoidable environmental risk for psychosis.
- Know who to contact.
It can be good to talk to someone, even when you are well, to voice your concerns and to have a good support system in place if you ever do feel you are having mental health issues you ll start from a much better place. This can be your school counsellor, your GP, or a registered psychologist.
There are many mental health services available to you in Australia, should you ever need it.
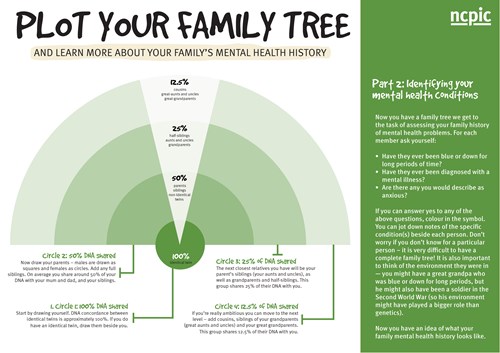
Plot your own family tree: activity
Click the thumbnail for a printable PDF.
References
Bhurgra, D. (2005). The global prevalence of schizophrenia. PLoS Medicine 2(5):e151
Bienvenu O.J., Davydow D.S., Kendler K.S. (2011). Psychiatric ‘diseases’ versus behavioural disorders and degree of genetic influence. Psychological medicine 41(1):33-40.
Cariaga-Martinez A., Saiz-Ruiz J., Alel -Paz R. (2016). From Linkage Studies to Epigenetics: What We Know and What We Need to Know in the Neurobiology of Schizophrenia. Frontiers in neuroscience 10: 202
Davis J., Eyre H., Jacka F.N., Dodd S., Dean O., McEwen S., et al. (2016). A review of vulnerability and risks for schizophrenia: Beyond the two hit hypothesis. Neuroscience and biobehavioral reviews 65: 185 94.
Gejman P.V., Sanders A. R., Duan J. (2010). The Role of Genetics in the Etiology of Schizophrenia. The Psychiatric clinics of North America 33(1): 35-66
Gibbs M., Winsper C., Marwaha S., Gilbert E., Broome M., Singh S.P. (2015) Cannabis use and mania symptoms: a systematic review and meta-analysis. Journal of affective disorders 15(171) :39-47
Griffiths A.J.F, Miller J.H., Suzuki D.T., et al. (2000). An Introduction to Genetic Analysis. New York: W. H. Freeman, 7th edition.
Johnson S.B., Blum R.W., Giedd J.N. (2009) Adolescent maturity and the brain: the promise and pitfalls of neuroscience research in adolescent health policy. The Journal of adolescent health 45(3):216-21
Kelley M.E., Wan C.R., Broussard B., Crisafio A., Cristofaro S., Johnson S., Reed T.A., Amar P., Kaslow N.J., Walker E.F., Compton M.T. (2016). Marijuana use in the immediate 5-year premorbid period is associated with increased risk of onset of schizophrenia and related psychotic disorders. 171(1-3):62-7
Kleibl Z., Kristensen V.N. (2016). Women at high risk of breast cancer: Molecular characteristics, clinical presentation and management. Breast 28: 136-44
Lamers F., Cui L., Hickie I.B., Roca C., Machado-Vieira R., Zarate C.A., Merikangas K.R. (2016). Familial aggregation and heritability of the melancholic and atypical subtypes of depression. Journal of affective disorders 204: 241-246
Livingston W.S., Rusch H.L., Nersesian P.V., Baxter T.3., Mysliwiec V, Gill J.M. (2015). Improved Sleep in Military Personnel is Associated with Changes in the Expression of Inflammatory Genes and Improvement in Depression Symptoms. Frontiers in Psychiatry 30(6):59
Marconi A., Di Forti M., Lewis C.M., Murray R.M., Vassos E. (2016). Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. Schizophrenia Bulletin pii: sbw003.
Matamura M., Tochigi M., Usami S., Yonehara H., Fukushima M., Nishida A., Togo F., Sasaki T. (2014). Associations between sleep habits and mental health status and suicidality in a longitudinal survey of monozygotic twin adolescents. Journal of sleep research 23(3):290-4
Monk, R. (2001). Bertrand Russell: 1921-1970, The Ghost of Madness. Free Press.
Russel, B. (1967). The Autobiography of Bertrand Russell. London, Allen & Unwin.
Russell, B., Griffin, N. (2001). The Selected Letters of Bertrand Russell, Volume 2: The Public Years 1914-1970. Psychology Press.
Scaini S., Belotti R., Ogliari A., Battaglia M. (2016) A comprehensive meta-analysis of cognitive-behavioral interventions for social anxiety disorder in children and adolescents. Journal of anxiety disorders 42: 105-112.
Shimada-Sugimoto M., Otowa T., Hettema J.M.(2015) Genetics of anxiety disorders: Genetic epidemiological and molecular studies in humans. Psychiatry and clinical neurosciences 69(7):388-401.
Slade T, Johnston A., Browne M.A., Andrews F., Whiteford H. (2009). 2007 National Survey of Mental Health and Wellbeing: methods and key findings. The Australian and New Zealand journal of psychiatry 43(7):594-605.
Smoller J.W., Finn C.T. (2003) Family, twin, and adoption studies of bipolar disorder. American journal of medical genetics 123C(1): 48-58.
Stein D.J., Phillips K.A., Bolton D, Fulford K.W., Sadler J.Z., Kendler K.S. (2010). What is a mental/psychiatric disorder? From DSM-IV to DSM-V. Psychological Medicine 40(11):1759-65
Waldfogel J., Craigie T.A., Brooks-Gunn J. (2010) Fragile families and child wellbeing. Future child 20(2):87-112.
Wray N.R., Gottesman I.I. (2103). Using summary data from the Danish national registers to estimate heritabilities for schizophrenia, bipolar disorder, and major depressive disorder. Frontiers in genetics 3: 118.